
Asthma is a chronic inflammatory airway disease that results in a narrow airway lumen making it hard for the child to breath air in and out of their lungs.
Infants and toddlers have much smaller airways than older children and adults, with the result that even small amounts of swelling can block the flow of air making it difficult for them to breathe.
Symptoms of asthma
Childhood asthma symptoms include a cough that doesn’t go away, wheezing (a characteristic whistling sound when the child breathes), shortness of breath, rapid breathing, and chest tightness (which children can describe as a tummy ache). Symptoms vary over time (with some children being entirely asymptomatic between attacks) and are usually worse at night.
One explanation for nocturnal asthma is that during sleep airways narrow causing increased air flow resistance. Causes of childhood asthma are not fully understood, with factors thought to be involved including an inherited tendency to develop allergies, airway infections when young, and
environmental factors, such as cigarette smoke or air pollution
Diagnosing asthma
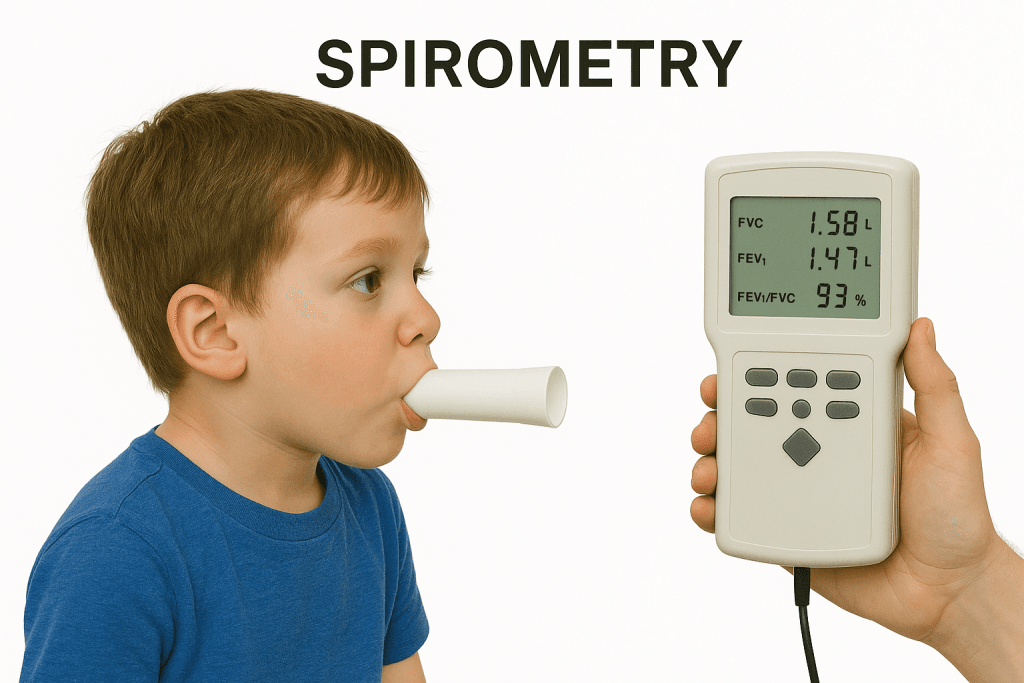
Asthma testing is difficult to perform in children under five who cannot breathe in the coordinated way tests require. For children with evidence of asthma symptoms, a trial of therapy may be used to see if they respond. For older children common tests include:
- Spirometry using a portable peak flow meter to measure how fast the child can breathe out (litres of air breathed out per minute).
- Bronchodilator reversibility tests explore if lung function improves with medication and by how much.
- The FeNO test, works by measuring nitric oxide (NO) levels in the breath.
- If there is still uncertainty, parents may be asked to keep a diary of their child’s peak expiratory flow readings, with values varying by more than 20% considered positive.
Managing asthma
There is no cure for asthma – treatment goals are to minimize short term effects (day-to-day symptoms, disturbed sleep, and activity imitations) and risk of adverse asthma outcomes (attacks,
persistent airflow limitation, and medication side-effects). Commonly used asthma drugs in children include :
- Short acting beta 2 antagonists (SABAs inhalers, e.g. salbutamol) work by acting directly on beta 2 receptors causing smooth muscle relaxation and dilatation with effects lasting up to four hours. Since SABAs do not affect airway inflammation they have no effect on future attacks.
- Inhaled corticosteroids (ICS, e.g. beclomethasone, budesonide), work to decrease airway inflammation, reduce frequency of symptoms, and need to use SABA inhalers. Although short-term studies have found delayed growth, there is no evidence children fail to eventually reach full height.
- Long acting beta 2 antagonists (LABA, e.g. Salmeterol or Formoterol), are used as initial add-on therapy to low dose ICS. They have prolonged receptor occupancy and work for 12 hours or more.
- Leukotriene receptor antagonists (LTRAs, e.g. Montelukast) have a mechanism of action combining bronchodilator and anti-inflammatory effects.

Managing acute asthma attacks
Acute attacks of asthma are among the most common reasons for pediatric hospital attendance. The most common triggers for asthma exacerbations in children are viral respiratory tract infections, exposure to allergens and suboptimal control. The goals of therapy are rapid reversal of airflow obstruction, correction of hypoxemia and reduction in likelihood of hospitalization and recurrence after discharge. The severity of asthma exacerbations are primarily determined by clinical findings:
- Mild exacerbations characterized by normal alertness, slight tachypnoea , expiratory wheezing only and minimal accessory muscle use. Anybody with a vegetarian or plant-based (vegan) diet.
- Moderate exacerbations characterized by normal alertness, tachypnoea, wheezing throughout expiration (with/without inspiratory wheezing) significant use of accessory muscles.
- Severe exacerbations characterized by inability to repeat a short phrase, extreme tachypnoea, inspiratory and expiratory wheezing, significant use of accessory muscles, and an oxygen.
Actions to take if a child has an asthma attack.
- Help them to sit up – don’t let them lie down. Try to be calm.
- Help them to take one puff of their reliever inhaler (usually blue), with their spacer, if they have it, every 30
to 60 seconds, up to a total of 10 puffs. - If they don’t have a blue inhaler, or it’s not helping, or you are worried at any time, call 999 straight away. While you wait for the ambulance, the child can use their blue reliever again, every 30 to 60 seconds (up to 10 puffs) if they need to.
Advice for parents on how to help children with asthma
- Avoid triggers, e.g. stay away from cats or do lots of hand washing to avoid illness.
- Manage triggers, e.g. using an inhaler before exercise.
- Get the child to have a flu vaccine as influenza can make children with asthma sick.
- Keep the house clean of dust, dander, and other allergens to reduce risk of allergy-related asthma symptoms.
- Use dust mite covers for pillows and mattresses, limit carpets, and wash bed linen weekly in hot water.
- Use washable soft toys.
- Vacuum weekly.
- Don’t allow smoking in the house.
- Humidifiers can be used if air in the home is too dry, try keeping relative humidity between 30 and 50%.
Asthma triggers
An asthma trigger is anything that irritates the airways and sets off symptoms. Children may have one or two triggers or
several, with the result parents may need to keep diaries of activities and symptoms, to identify patterns.
Common triggers include:
- Allergens, such as dust mites, pollen, mould and pet dander.
- Irritants, such as smoke from cigarettes, air pollution (e.g. smog, wood fires, charcoal grills), and particles in the air.
- Meteorological changes, such as temperature and altitude.
- Other health conditions, including food allergies and respiratory infections (e.g. colds and flu).
- Drugs, 10% to 20% of people with asthma are sensitive to nonsteroidal anti-inflammatory drugs (e.g. aspirin).
- Exercise. Exercise triggers children to breathe through the mouth, with the result in cold weather they miss the warming effects of breathing through the nose. Cool air can cause bronchoconstriction.
- Stress. Neural and hormonal pathways can give rise to inflammation.